Multiple Thoracolumbar Fractures
A 55-year-old male patient was referred from another hospital 5 days after a work accident. Surgery had been recommended for T11 and L1 fractures seen in the lumbar plain radiograph, CT, and MRI scans.

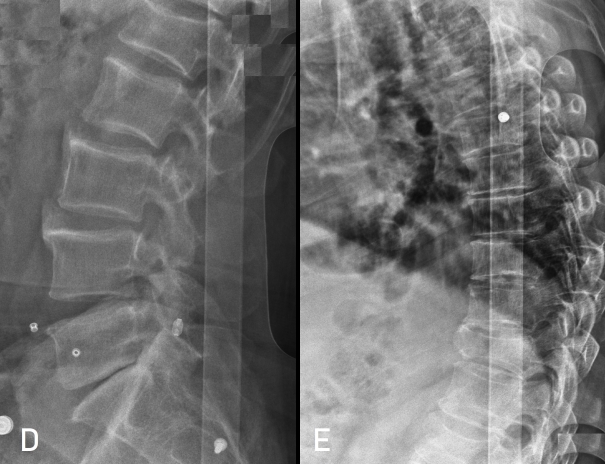
Figure 1 & 2: Height loss in T11 and L1 vertebrae is observed in plain radiograph, CT, and MRI examinations. Height loss in T11 is more prominent, close to 50%. CT sections do not include the T11 level. In the T1-weighted MRI scan (B) in the upper center, there is a hypodensity in the upper half of the L5 vertebral body that could also be a fracture. STIR sequences are missing in the examination.
The patient, who was immobilized, had a good general condition, stable vital signs, and a normal neurological examination. He had widespread and severe back and low back pain. Physical examination was normal except for tenderness on palpation in the back and low back. Since the lumbar MRI examination was incomplete (no STIR sequence), the T11 vertebra was fractured, and the entire back region was painful, a new thoracic and lumbar MRI was requested.
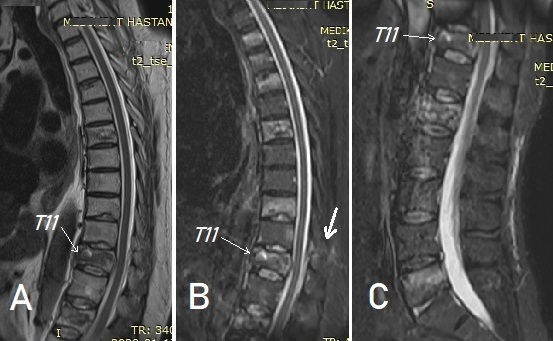
Figure 3: In thoracic and lumbar MRI examinations, fractures are visible in a total of 8 vertebrae, most prominently in STIR sequences (B and C): T2, T3, T4, T6, T9, T11, L1, and L5. Additionally, fracture in the posterior elements and partial ligament injury are seen at the T11 level (B, thick arrow).
Fractures were detected in a total of 8 vertebrae (T2, T3, T4, T6, T9, T11, L1, and L5). After discussing with the patient and his relatives, a decision for surgery was made.
SURGERY
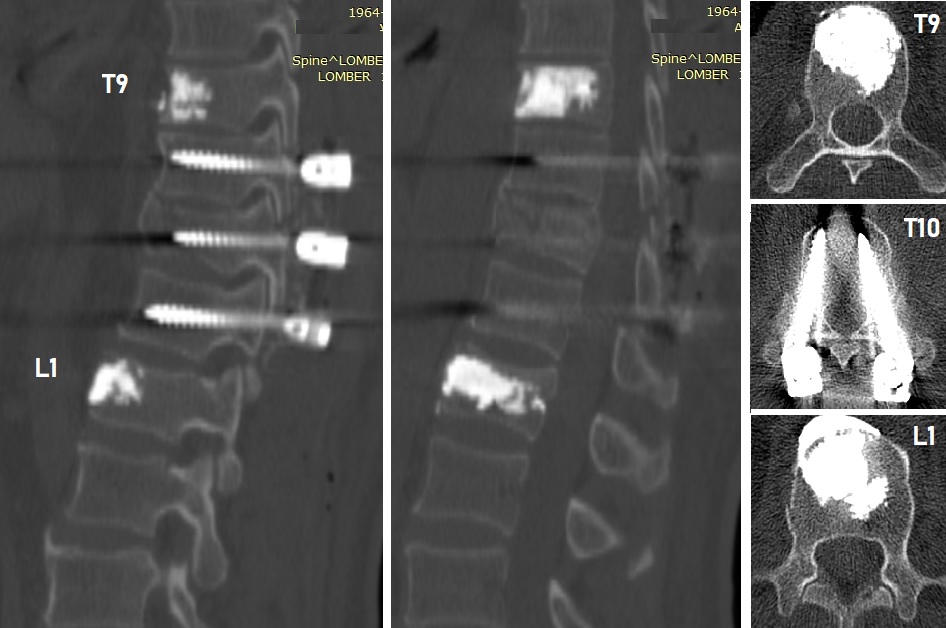
Figure 4: Postoperative plain radiographs show T9 and L1 kyphoplasty and T10-11-12 transpedicular stabilization.
Kyphoplasty (6 ml methylmethacrylate each) was performed on the T9 and L1 vertebrae, and transpedicular stabilization was applied to the T10-11-12 vertebrae. The laminae and facets were partially decorticated, and fusion-enhancing material (Ca-phosphate granules) and autogenous bone taken from the area were laid. It was observed that the T11 lamina and facet joint were fractured bilaterally. Laminectomy was not performed.
No procedure was performed on the other fractured vertebrae T2, T3, T4, T6, and L5; they were followed up.
The patient was mobilized uneventfully with a TLSO corset the morning after surgery and was discharged on the second postoperative day. He has no problems in the short-term follow-up.