Discogenic Low Back Pain
A 40-year-old female patient presented with complaints of low back pain and occasional left leg pain. The patient, a housewife, stated that her low back pain started 4 years ago, she did not benefit from various physical therapy sessions and medication, and she could no longer maintain her daily life normally due to the pain. At the time of presentation, she was 1.74 m tall and weighed 68 kg. It was determined that she had lost weight and performed back exercises as advised, but these measures were insufficient to alleviate the pain.
The patient's examination revealed no findings other than local tenderness upon palpation in the lumbar region. She described a dull low back pain that increased with bending forward, radiated to both sides of the back, eased with lying down, and worsened with sitting. The severity of low back pain was measured as 6 out of 10 on the VAS (Visual Analog Scale). Her neurological examination was normal.
MRI (Magnetic Resonance Imaging) examination showed blackening of the L4-L5 disc and an annular tear at this level. No signs of instability were found in her functional plain radiographs.

Figure 1: In the patient's T2-weighted lumbar MRI examination, the L4-L5 disc is seen to have blackened due to the decrease in water content caused by degeneration. A high intensity zone (HIZ) is observed at this level, appearing as a punctate bright signal in the posterior annulus fibrosus, which is consistent with an annular tear.
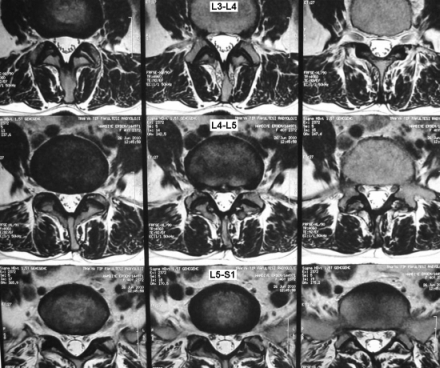
Figure 2: T2-weighted axial MRI sections show no significant disc herniation or foraminal stenosis, but a high signal intensity is present in the annulus at the L4-L5 level.
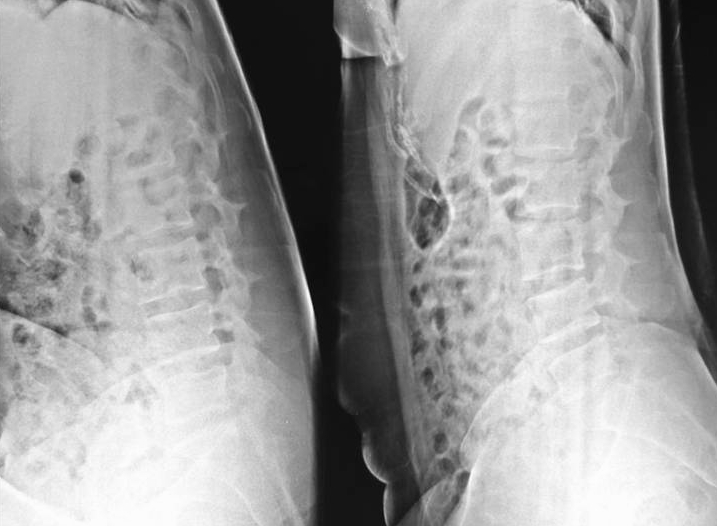
Figure 3: No signs of instability were found in the patient's functional (flexion/extension) radiographs.
Surgery
Following the necessary consultations and information, a consensus was reached, and the decision for surgery was made. The patient underwent L4-L5 transpedicular stabilization. Given the patient's young age, fusion was not targeted, and dynamic screws were used. Postoperative images are presented below. The patient, who developed no complications, rapidly improved her pain and was discharged from the hospital on the third postoperative day. The patient, who is still under our follow-up, continues her daily life without problems in the 1st postoperative year (VAS score: 0-1) and does not require pain medication.
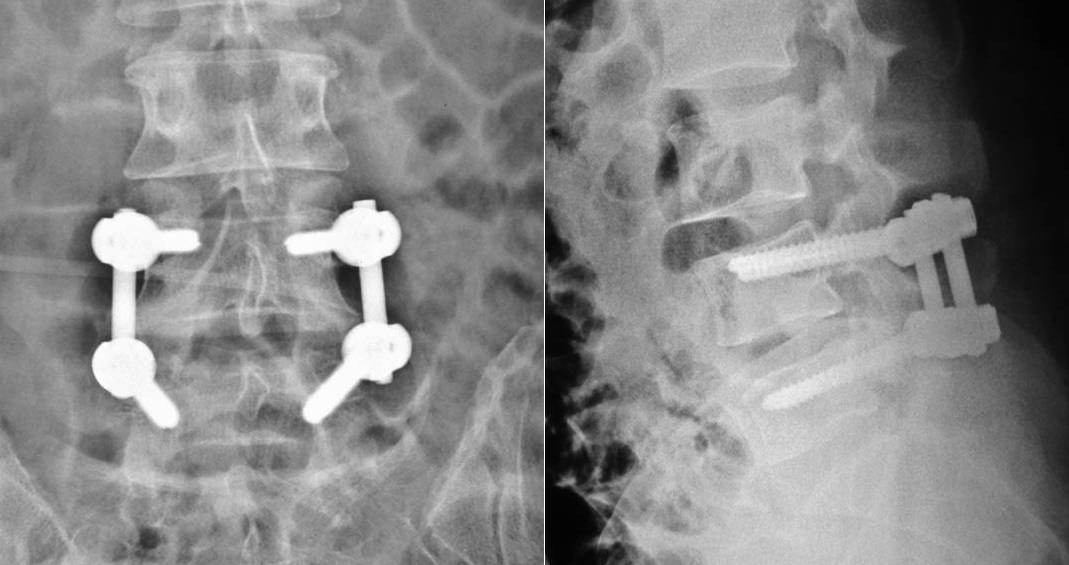
Figure 4: L4-L5 dynamic stabilization. Dynamic screws are visible in the postoperative radiograph.
Comment
This patient is a typical example of lumbar discogenic pain. The patient's pain increases with spinal loading (sitting, standing, and bending forward), radiates like a belt around the back to the sides, and decreases with lying down. The MRI examination shows that the L4-L5 disc is degenerated and has a tear in the annulus. All these findings support the L4-L5 disc as the source of pain. The most definitive way to confirm this diagnosis is provocative discography. This option was discussed with the patient and deemed unnecessary. Classical options in the treatment of a symptomatic, non-herniated disc are: conservative treatment (medication, rest, physical therapy, weight loss, and exercises), intradiscal procedures (nucleoplasty, etc.), and fusion. In this patient, conservative treatments failed, and an intervention was necessary. Intradiscal procedures have low success rates, and fusion surgeries have relatively high complication rates in the short and long term.
The dynamic fixation treatment applied to our patient is a relatively newer technique. It involves partial immobilization in the instrumented L4-L5 segment, allowing restricted movement (semi-rigid) but reducing painful excessive movements and disc loading. The screw used in our patient is a screw-based dynamic system that allows movement in the sagittal plane (flexion/extension) through a joint between the screw head and the body. Dynamic systems are diverse, and it cannot be said that sufficient studies have been conducted on all of them regarding their safe use. Their worldwide use varies regionally, and opinions about them are diverse. In Turkey, the SSI (Social Security Institution) allows the use of these systems under the age of 45. Our results with screw-based dynamic systems are excellent in our patients, and we observe that they are beneficial in appropriately selected cases.