Transforaminal Epidural Injection for Low Back and Leg Pain due to Lumbar Disc Herniation
A 45-year-old male patient presented with pain radiating to the middle of the low back, hips, and groin. He stated that his long-standing pain had increased in the last six months.
There was no loss of muscle strength in the patient's neurological examination. Reflexes were normal. Hypesthesia was detected in the S1 dermatome on the right. Local tenderness was found on palpation over the upper part of the sacrum and at the Valleix points on the right (midpoints on the posterior aspect of the hip, thigh, and calf). His lumbar MRI examination is shown below.

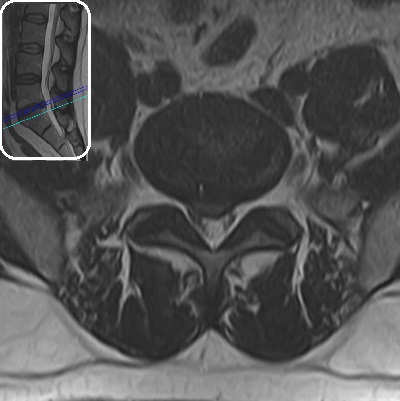
Figure 1: Lumbar MRI examination shows a central bulging at the L5-S1 level. Although a small opening in the annulus fibrosus and a small extruded fragment touching the right S1 root might be suspected, it cannot be said definitively. Hypointensity within the disc and degenerative signal changes in the anterior part of the lower endplate of the adjacent L5 vertebra are observed at the same level (degenerative disc disease). Lumbar lordosis is preserved. No significant problems were detected in other disc levels, facet joints, and paravertebral muscles.
The patient's complaints were attributed to this level due to the intensity of degeneration at the L5-S1 level, significant bulging, findings suggesting S1 root compression or irritation (S1 dermatome hypesthesia and tenderness at Valleix points), and local pain. Groin pain, which is among the patient's complaints, is not a typical finding in lumbar problems between L3-S1. Hip joint and sacroiliac joint problems should also be suspected. However, the patient's examination was found to be normal in these respects. Since our clinical experience suggests that groin pain can occur in L5-S1 disc pathologies, no additional imaging was planned in this direction, and treatment for L5-S1 discopathy was planned.
Treatment
Due to the long-standing pain that had been ongoing for 6 months, an interventional treatment was considered instead of continuing with medication or physical agents. Since there was no large disc herniation and no neurological finding other than S1 dermatome hypesthesia, discectomy was not indicated at this stage. The patient was informed about treatment possibilities, and a joint decision for epidural injection was made. A right transforaminal epidural injection was administered to the patient. Below are the X-ray images taken during the procedure and the details of the procedure.
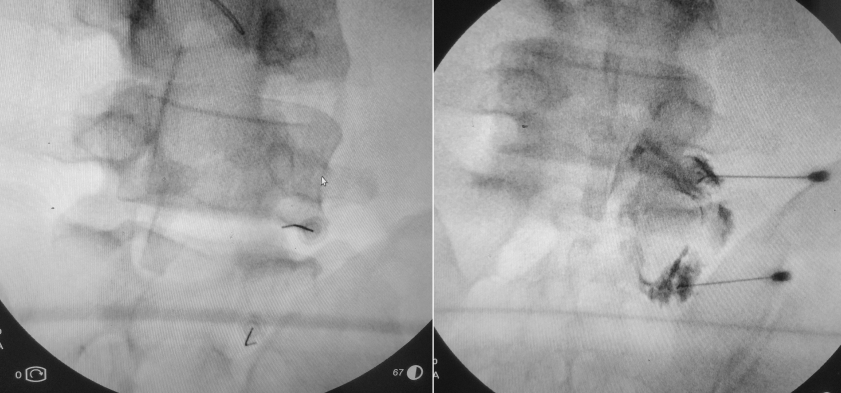
Figure 2: Application of epidural injection via the right L5-S1 foramen and S1 foramen.
The injection was performed in the operating room, with the patient in the prone position with the abdomen supported, under fluoroscopy and contrast medium control (300 mg/ml Ultravist), using 20G thickness and 9 cm long spinal needles with a sterile technique. A total volume of 20-30 ml mixture containing 1% adrenaline-free Lidocaine + saline + ½ ampoule of depot steroid was administered. The infraneural technique was used at the L5-S1 level. The image on the right shows appropriate contrast passage to the epidural space from both foramina. For better pain control, right L2-S1 medial branch blocks were also performed in the same session.
Result
No complications were observed during or after the procedure. The patient was walked one hour after the procedure and was discharged without any problems. In the control examination performed three weeks later, the patient stated that his pain had decreased by 80%, he did not use painkillers after the first week following the procedure, and his current pain did not disrupt his sleep or daily activities.
No other treatment was considered at this stage, and the patient was followed up with the recommendation to apply again if his complaints increased. He was advised not to gain weight and to perform exercises to strengthen his abdominal and back muscles. There are no problems in the three-month follow-up.
Comment
In this patient, we encountered degenerative disc disease limited to a single lumbar level and a disc herniation at the stage where the annulus fibrosus was not yet fully torn (bulging). Adequate pain control was achieved with the epidural injection. The possibility of surgical intervention was pushed to the background at this stage due to the absence of significant neurological loss. Indeed, epidural injection gives satisfactory results in most patients. However, it should not be forgotten that the injection performed consists only of pain treatment, the existing degenerated disc cannot be repaired, and problems may be experienced from the same level in the future with the progression of anatomical deterioration.