Cervical Myelopathy in Klippel-Feil Syndrome
A 31-year-old female patient presented with complaints of neck pain, stiffness, and rigidity in her body that had increased over the past year. Neurological examination revealed hyperactive deep tendon reflexes and an extensor plantar response. Direct radiographs and Magnetic Resonance Imaging (MRI) showed multi-level congenital fusion in the cervical vertebrae, signs of instability at the C3-C4 level, spinal cord compression, and signal changes in the spinal cord at this level.

Figure 1: Flexion/extension radiographs show fusion of the C2-C3 and C4-C5-C6 vertebrae. At the unfused C3-C4 level, shifting is seen on flexion/extension radiographs, and a pronounced angulation is seen at the C6-C7 level, but no shifting is present.
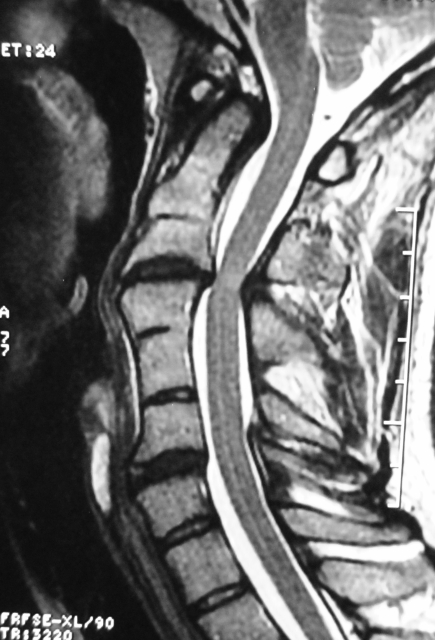
Figure 2: Cervical MRI shows anterior and posterior compression of the spinal cord at the C3-C4 level, and signal changes in the spinal cord at this level.
Decompression and stabilization were planned at this level due to obvious signs of myelopathy and instability at the C3-C4 level.
Surgery
The patient underwent C3-C4 interlaminar decompression (resection of the ligamentum flavum causing compression, along with the inferior half of the C3 vertebra and the superior half of the C4 vertebra) and stabilization with a posterior screw-rod system via a posterior approach. Fusion was targeted by grafting the C3-C4 facet joint with autogenous bone taken from the laminectomy area. Intralaminar screws were used at the C2 level, and lateral mass screws were used at the C5-C6 levels.
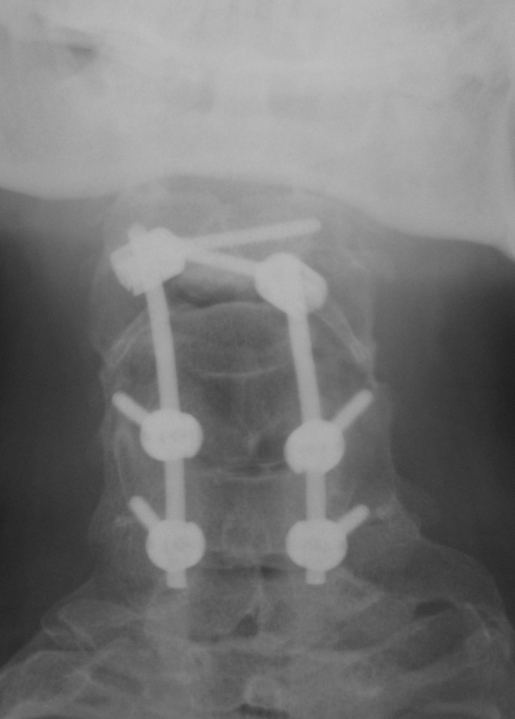

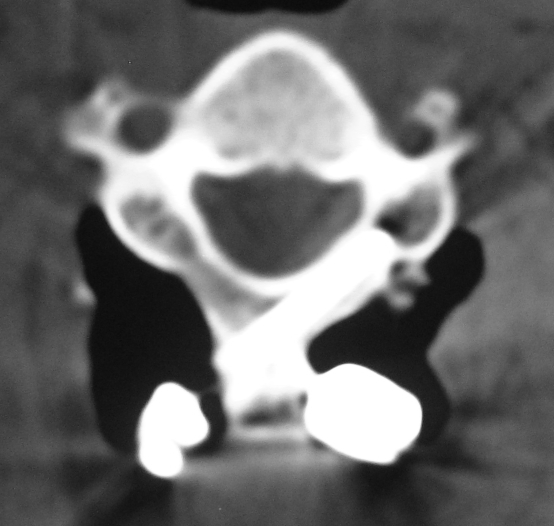
Figure 3: Postoperative plain radiographs show the stabilization system at the C2-C6 level. Intralaminar screws were used at the C2 level (rightmost image), and lateral mass screws were used at the C5-C6 levels.
Follow-up
No complications developed during the postoperative period. The patient reported a reduction in her complaints in the early period. At the 3rd-month neurological examination, there was a significant improvement in the signs of myelopathy. The patient is in her first postoperative year and remains under our follow-up.
Comment
Klippel-Feil syndrome is a congenital fusion of cervical vertebrae (and sometimes in other spinal regions). These findings are sometimes accompanied by a short neck and a low hairline. Since the load of movement shifts to the unfused disc levels, accelerated degenerative changes and instability and spinal cord compression, as seen in our case, can occur at these levels. In this case, decompression and stabilization could have been achieved with anterior or posterior techniques. Due to the low risk of complications and their benign nature, we preferred the posterior approach in our case. The C6-C7 level (the only unfused subaxial disc space) is a potential candidate for instability, which necessitates long-term, even lifelong, follow-up.